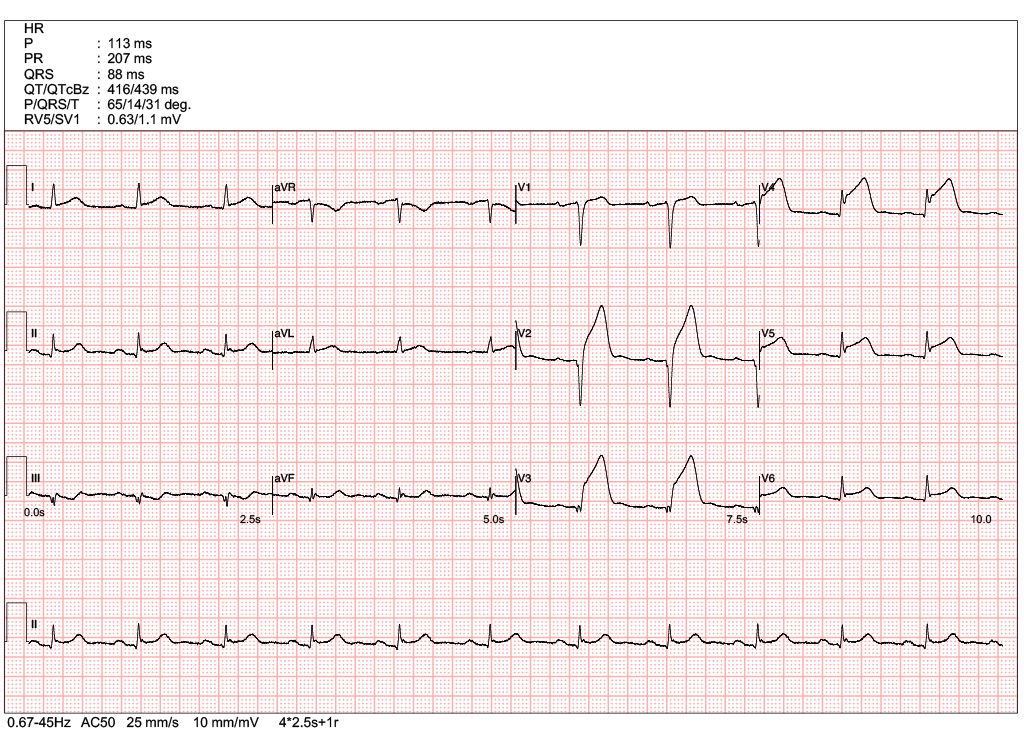
A 70-year-old man presented to the AED with acute chest discomfort and SOB. His BP was 110/50 mmHg and SaO2 was 96% on 1L oxygen.
Which of the following is the most appropriate next step in management?
Choose the correct answer.
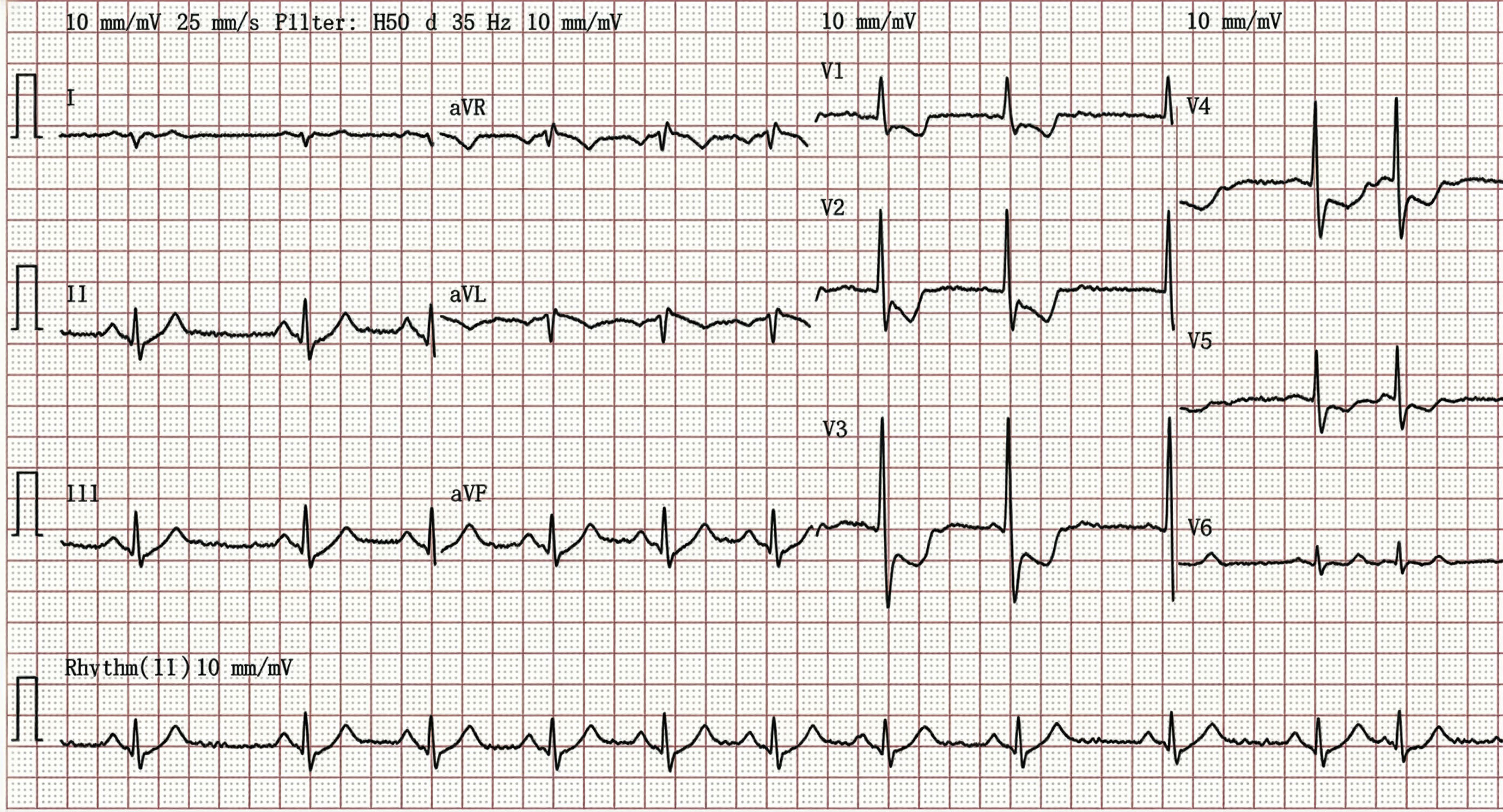
The ECG demonstrates ST-segment depression in leads V1–V3 with prominent R waves, a pattern highly suggestive of posterior STEMI. In such cases, the diagnosis could be further supported by evaluating the extended posterior leads V7–V9, which may reveal diagnostic ST elevation in some patients. Echocardiography provides crucial diagnostic verification when ECG findings remain equivocal. The most definitive finding is localized wall motion abnormality specifically involving the posterior segment of the left ventricle.
ST-T wave abnormalities associated with digoxin toxicity are usually diffuse and present across multiple leads, distinguishing them from the localized ischemic changes of a posterior infarction.
The most common ECG finding in pulmonary embolism (PE) is sinus tachycardia. In some patients, ECG findings may reflect acute right ventricular overload, manifesting as a new right bundle branch block (RBBB) or T-wave inversions in leads V1–V3, though significant ST-segment depression is less frequent. While the classic 'S1Q3T3' pattern (characterized by a deep S-wave in lead I, alongside a Q-wave and inverted T-wave in lead III) is suggestive of acute right heart strain, it is an infrequent finding with low sensitivity in clinical practice.
The presence of clearly identifiable P waves despite fluctuations in the atrial and ventricular rates is compatible with sinus arrhythmia rather than Atrial fibrillation.
A 50-year-old woman presented to the AED at 2:00 a.m. with palpitations and chest discomfort. Her BP was 90/50 mmHg and SaO2 99% on room air.
What is the most appropriate management?
Choose the correct answer.
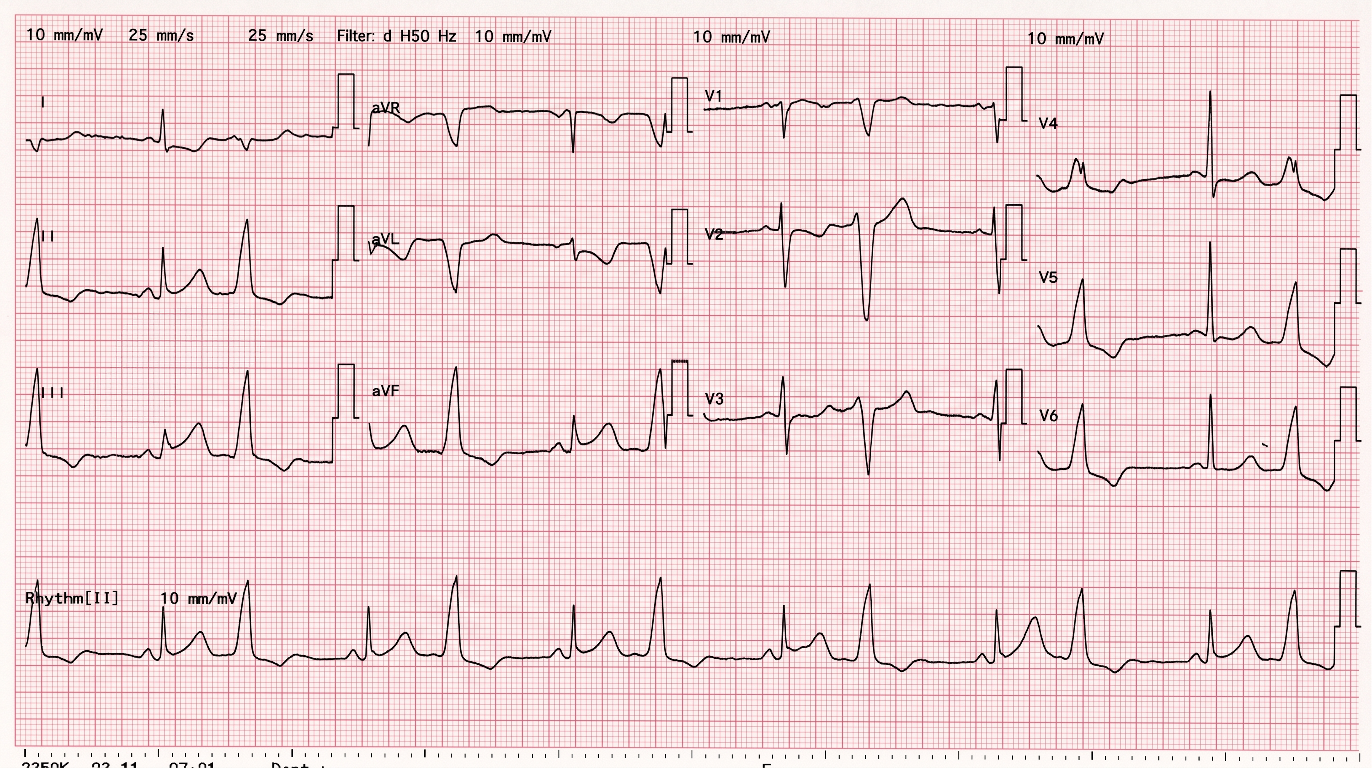
The ECG demonstrates sinus rhythm with frequent PVCs in a bigeminal pattern, which may distract from the primary rhythm.
Notable ST elevation is present in the inferior leads of the conducted QRS complexes, with reciprocal changes in V2-V5, diagnostic of an inferior STEMI.
Given the morphology, the premature complexes are likely of RV outflow tract origin.
Management of an acute STEMI requires emergent reperfusion therapy; primary PCI is the preferred strategy, though fibrinolytic therapy should be administered if PPCI cannot be performed within 120 minutes of medical contact.
A 90-year-old man presented with acute chest discomfort and SOB. He is a heavy smoker with a history of recurrent admissions for COPD exacerbations. His BP was 120/80 mmHg and SpO2 was 88% on room air.
Which of the following is the most appropriate next step in management?
Choose the correct answer.
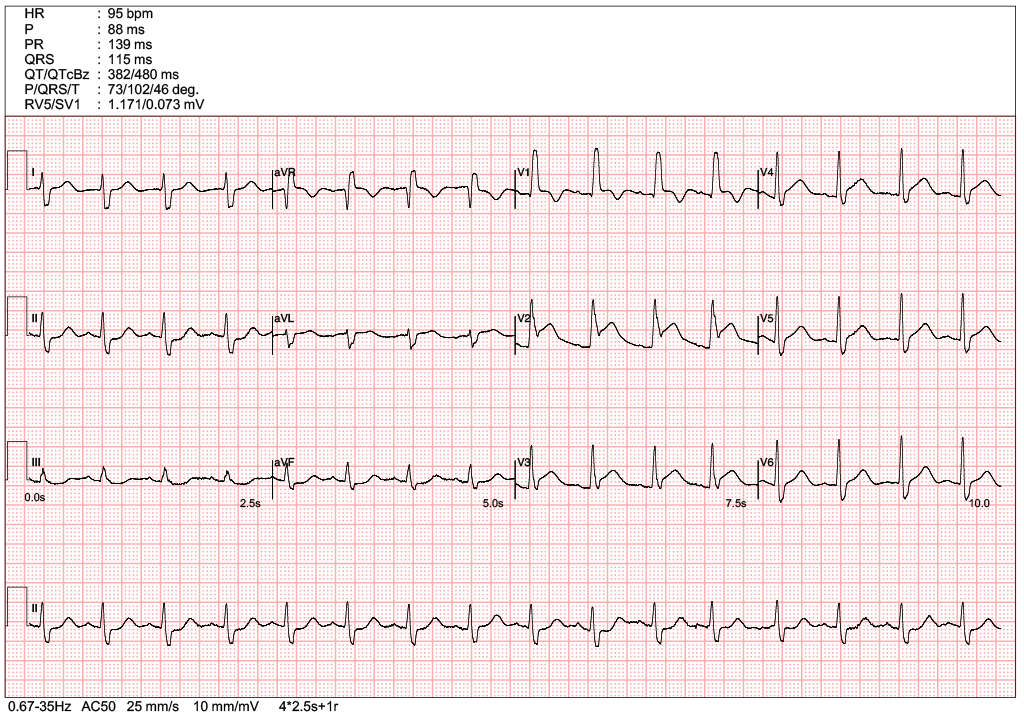
The ECG showed an RBBB with ST elevation in leads V1–V4, consistent with an anterior STEMI.
Patients with COPD and cor pulmonale—without acute myocardial infarction—should not exhibit ST elevation on the ECG. RV dilation in COPD patients can be attributed to cor pulmonale alone, even in the absence of a pulmonary embolism. A prolonged QTc without torsades de pointes does not warrant IV magnesium treatment
An 85-year-old man presented to the clinic with exertional dizziness and episodes of syncope. He is now homebound due to the severity of his symptoms. He also complained of mild shortness of breath (SOB) and lower limb swelling of several weeks' duration.
What is the most likely ECG diagnosis?
Choose the correct answer.
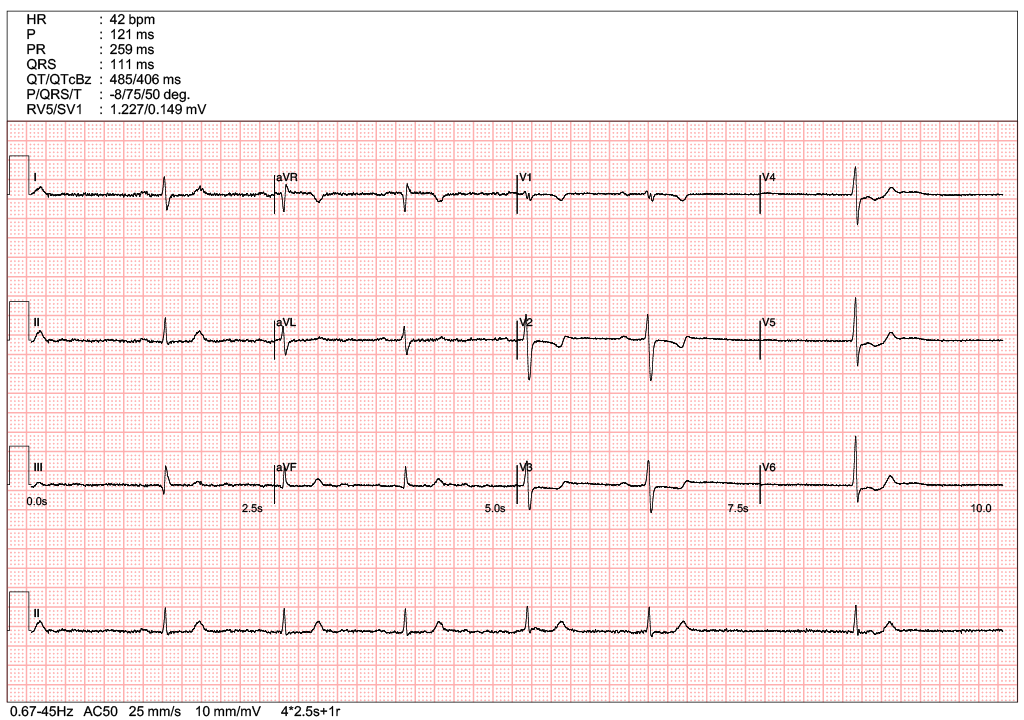
Initial rhythm is slow sinus rhythm with heart rate significantly below 60 bpm. There is clear sinus pause between the 5th and 6th complex in long lead II. The pause is not exactly multiples of previous P-P intervals, it suggests a sinus arrest rather than sinoatrial exit block. The last beat is a junctional escape beat with possibly a retrograde P wave.
A 60-year-old man presented to the AED with intermittent chest pain of several days' duration. He could not recall the exact onset of the pain. His BP was 150/90 mmHg and SpO2 was 97% on room air.
Which of the following statement is correct?
Choose the correct answer.
The ECG showed ST-segment elevation in the Anterior leads (V2-4), consistent with an Anterior STEMI.
Although the exact onset time was unknown, it should not be treated as a delayed presentation because the chest pain was intermittent and persistent. Baseline ECG comparison is not mandatory for a diagnosis of STEMI, and overt reciprocal changes are not always present. Since obvious ST elevation was present on the initial ECG, serial ECGs are not necessary, thereby avoiding delay in revascularization
